
Mammary Tumours In Felines
24th Oct 2025
October is breastfeeding cancer awareness month. Therefore, this month we will discuss how cats can be affected by mammary cancer, its diagnosis, prognosis and treatment.

Clinical Features
When thinking about clinically important features, one of the main concerns is the biological behaviour of the particular type of cancer. With feline mammary cancer, size does not matter!
A common question of both owners and vets (to pathologists and oncologists) is: “It’s only a small mass, how likely is it to be malignant/cancer?” At least 85% of feline mammary masses are malignant and this is very different from dogs, where many mammary masses are benign.
Also, while many feline mammary masses will be solitary, more than 60% of cats will have multiple masses and they can be related – meaning they can and are likely to have spread (via metastasis) from one mammary gland to another. One final aspect of biologic behaviour is that feline mammary masses tend to grow rapidly and are often not detected until they are more than 2 cm in diameter.
The probability of metastasis is another important clinical feature, as approximately 50% of feline mammary tumours will have regional lymph node involvement. Distant metastasis can also occur with spread to the lungs or pleura (lining of the lungs) and viscera (spleen, liver or other organs).
These features all highlight the importance of owner awareness for early detection, diagnosis and treatment to maximise the probability of a positive outcome.
Clinical Prognostic Factors
Clinical prognostic factors are characteristics associated with the course and outcome of cancer that can help predict a patient's prognosis. These factors are important for clinicians to assess the likely progression of the disease and guide treatment decisions. Prognostic factors can vary depending on the type and stage of cancer. The commonly considered clinical prognostic factors for feline mammary cancer include the following:
- Ulceration – if the mass is ulcerated, the prognosis is not as good, as if the overlying tissues are intact and not ulcerated.
- Size of the mass is associated with reported median survival times (the length of time it takes for 50% of affected cats to die of their disease) as shown in Table 1.
Table 1. Size of mammary mass and median survival time according to published studies.
|
Size |
Median survival time |
|
< 2 cm |
1.5 – 3 years |
|
2 – 3 cm |
2 years |
|
> 3 cm |
< 6 months |
Other clinical prognostic factors that are discussed below include:
- Clinical stage and lymph node metastasis (regional or distant) by itself
- Type of surgery
- Histological grade
It is important to remember that individual cases will vary and prognosis is an estimation based on statistical data reported in published research.
Staging
Cancer staging is a standardised way of describing the extent of a cancer's spread that helps in planning appropriate treatment and predict a patient's prognosis. Staging systems vary depending on the type of cancer, but the most commonly used system is the TNM staging system.
The TNM system provides a detailed description of the primary tumour (T), regional lymph nodes (N), and distant metastasis (M). Staging allows for consistent communication among healthcare professionals and researchers. Different types of cancer may have specific staging systems tailored to their characteristics and patterns of spread. As research advances, staging systems may be refined to guide treatment decisions and provide more accurate prognostic information (Table 2).
The following observations/procedures may be required for staging (see arrow), starting from the left and working towards the right (arrow head) although not all may necessarily be needed in every case. However, lack of any staging can lead to unrealistic expectations of owners. A conservative surgical approach combined with a lack of staging has a negative impact on prognosis.
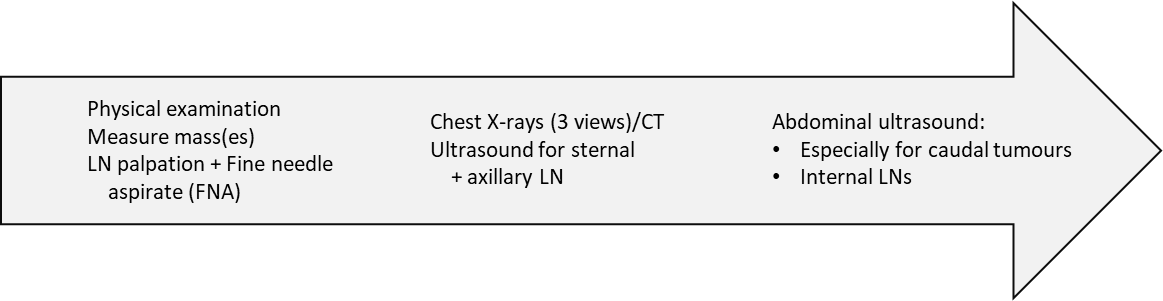
Table 2. The TNM clinical staging system for feline mammary tumours modified from the WHO (World Health Organization) with published survival times.
|
Clinical stage |
Tumour diameter (T) |
Regional lymph node involvement (N) |
Distant metastasis (M) |
Median survival time in months (MST) |
|||
|
I |
< 2cm |
(T1) |
Negative |
(N0) |
Negative |
(M0) |
29 |
|
II |
2 – 3 cm |
(T2) |
Negative |
(N0) |
Negative |
(M0) |
12.5 |
|
III |
> 3 cm ≤ 3 cm |
(T3) (T1 – T2) |
Negative/Positive Positive |
(N0) (N1) |
Negative |
(M0) |
6 9 – 11 |
|
IV |
Any |
(Any T) |
Either |
(Any N) |
Positive |
(M1) |
3 - 10 |
Tumour size and presence of metastasis to regional lymph nodes (see Box) or distant sites all have prognostic implications and this is why staging is needed prior to surgery. Any suspicious LNs or organs should be checked with fine needle aspiration (FNA) for cytology or biopsy for histopathology to confirm metastasis.
Diagnosis
Another common question is whether cytology after a fine needle aspiration (FNA) of a mammary mass is useful? Since most feline mammary masses are malignant, FNA and cytology is rarely used by vets. Histology is needed for definitive prognosis (histopathology of the excised mass once surgery is completed). However, cytology can be useful for the pet owner – to confirm that it is mammary neoplasia, to justify staging or the need for aggressive surgery – as it allows appropriate planning from the start. Also, non-mammary feline neoplasia is rare so, if a cat is entire, cytology could rule out mammary neoplasia (e.g. if there is an inflammatory cause).

Surgical Approach and Prognosis
The type of surgery carried out is an independent prognostic factor for median times to recurrence and survival: a radical bilateral mastectomy with removal of affected/suspected lymph nodes gives the best prognosis (Figure 2). The radical bilateral surgery technique involves an en bloc resection with lateral margins of 2 – 3 cm and removal of fascia at least in area of potential recurrence (i.e. below the mass). The current recommendation is to do one procedure rather than two unilateral procedures 4 weeks apart.
Type of surgery is associated with prognosis (Table 3): there is a 20% recurrence rate with bilateral surgery vs 47% with unilateral surgery. Local resection is associated with 70% recurrence or new lesions/metastases in LNs and narrow/incomplete margins carry the highest risk. Radical bilateral mastectomy is protective against progression (spread after surgery) as the mammary glands (± LNs) are removed. However, if metastasis is present before surgery, there is no difference between unilateral and bilateral surgery. This further highlights the importance of staging before surgery, as mastectomy is not protective beyond the mammary glands.
Table 3. Type of surgery is associated with median times to recurrence (disease-free interval) and survival:
|
Type of surgery: |
Bilateral |
Unilateral |
Regional |
Mastectomy |
|
Disease- free interval: |
18 – 30 |
10 - 18 |
7 |
months |
|
Median survival time: |
37 |
15.5 |
months |

Figure 2. Showing radical bilateral mastectomy.
Histopathology and prognosis
All tissue removed at surgery should be sent to a laboratory for histopathological examination. However, the histological grade of the mammary mass(es) has limited usefulness with respect to predicting prognosis as most of the evidence is based on retrospective studies that used surveys and limited clinical information as to stage or follow-up.
Thus, the reported survival times in Table 4 are low – likely from studies that included cats having undergone marginal/regional surgeries (not radical surgery). In spite of this, histopathology can also give important information about prognosis based on evidence of: vascular/lymphatic invasion as a potential indicator of metastasis post-op if no mets were detected during pre-op staging and this carries a worse prognosis; tumour type is also important as tubulopapillary masses tend to have longer survival times compared to anaplastic adenocarcinomas that tend to have shorter survival times. Histopathology of any removed lymph nodes is also important to assess spread to LNs removed during surgery.
|
Grade |
Median survival time |
|
I * |
29 – 31 months |
|
II |
12 months |
|
III |
0 months |
* Only about 20% of cases were grade I (100% had 1-year survival)
Chemotherapy
After radical bilateral surgery, chemotherapy may be used to treat potential microscopic disease and this is indicated if vascular invasion or metastasis is present (although it is best to remove any affected LNs first). The role of post-op chemotherapy is unclear if there are positive prognostic indicators: radical bilateral mastectomy, clear LNs, no sign of vascular/lymphatic invasion on histopathology and low histopathological grade of the mammary mass(es).
Post-op chemotherapy may be protective if negative prognostic factors are present: if it is an anaplastic adenocarcinoma or there is vascular/lymphatic invasion evident on histopathology of the removed tissues. Metronomic chemotherapy using low doses of cyclophosphamide continuously over a long period of time to modulate the tumour microenvironment (TME) due to the combination of cytotoxic, antiangiogenic and immunomodulatory effects.
Chemotherapy after conservative surgery such as local or regional resection, does not avoid recurrence or metastasis, it merely delays it. There is scarce information available on the effectiveness of chemotherapy to treat macroscopic disease (metastasis): multi-agent chemotherapy only gives a short-lived (< 3 months) response in 20-30% of cases.
Conclusions
- Approximately 85 – 95% of feline mammary tumours are malignant.
- The only prognostic factors we can control are early detection and type of surgery (radical, bilateral)
- Lack of staging can lead to unrealistic owner expectations, inappropriately planned surgery and worse prognosis. Thorough staging prior to surgery is needed to detect disease beyond the mammary glands and regional LNs.
- Early detection and radical surgery are extremely important to improve survival. There is low recurrence and development of distant metastases after bilateral mastectomy while a conservative surgical approach has a negative impact on prognosis.
For any disease, albeit in humans or animals, it is important to be vigilant and check for any possible signs, or bodily changes, so that any concerns can be investigated as soon as possible.
In particular, as for any cancers, the earlier the detection, the higher the chances of survival.
The content of this information sheet does not constitute advice and should not be relied upon in making or refraining from making, any decision. ACT recommends discussing this with your vet practice.
- Adapted from a presentation at the London Vet Show November 2023 by Ana Lara Garcia DVM PGCert MSc PhD Dip ACVIM & ECVIM-CA (Oncology) Oncology Consultant, IDEXX UK & Spain